Übersetzt aus dem Englischen:
Lernen Sie die chirurgische Technik zur Tibiakopf-Fraktur: 360-Grad-Zugang, anteriore Vorgehensweise (Stufe 2), variable Winkel proximale Tibiaplatte (DePuy-Synthes) mit schrittweisen Anweisungen auf OrthOracle. Unsere E-Learning-Plattform enthält hochauflösende Bilder und eine zertifizierte Fortbildung (CME) des chirurgischen Verfahrens zur Tibiakopf-Fraktur: 360-Grad-Zugang, anteriore Vorgehensweise (Stufe 2), variable Winkel proximale Tibiaplatte (DePuy-Synthes).
Wie bei vielen Traumata im Erwachsenenalter haben Tibiakopf-Frakturen eine bimodale Verteilung. Bei jüngeren Patienten resultieren diese Verletzungen aus hochenergetischen Mechanismen wie Stürzen aus großer Höhe oder Verkehrsunfällen, während sie in der älteren Bevölkerung häufiger durch einfache Stürze verursacht werden.
Tibiakopf-Verletzungen wurden von Schatzker auf der Grundlage von Röntgenaufnahmen in 6 Typen eingeteilt. Typen 5 (bikondylär) und Typ 6 (bikondylär mit vollständiger Trennung der Gelenkfläche von der Tibiaschafthülle) stellen die hochenergetischen Verletzungen dar. Eine neuere Klassifikation von Luo, basierend auf CT-Scans, unterteilt den Tibiakopf in 3 Säulen, medial, lateral und posterior, und hilft, die chirurgische Vorgehensweise bei der Fraktur je nach genauer Frakturkonfiguration zu leiten.
Die Mehrheit der Tibiakopf-Frakturen betrifft die laterale Seite und kann mit dem Standard anterolateralen Zugang mit Meniskusanhebung angegangen werden. Für Frakturen mit medialer oder posteriorer Beteiligung sind weitere Zugänge möglich, darunter direkter medialer, postero-medialer, direkter posteriorer oder sogar posterolateraler Zugang. Die Fixierung bikondylärer Tibiakopf-Frakturen über einen einzelnen anterioren Mittellinien-Schnitt wird heutzutage im Allgemeinen vermieden, da hierfür eine umfangreiche Weichteildissektion erforderlich ist und die damit verbundenen Wundprobleme.
Original Intro:
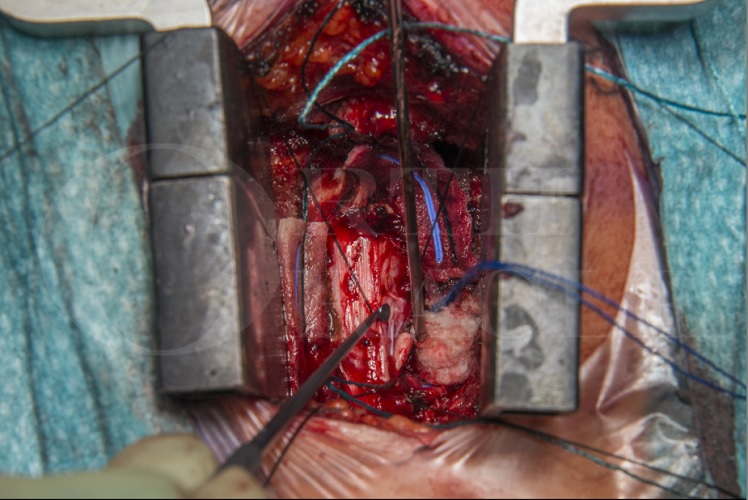
Posterior Cervical Laminoplasty (Bioplate cranial fixation system) and Excision Of C5 nerve sheath tumour
Learn the Posterior Cervical Laminoplasty (Bioplate cranial fixation system) and Excision Of C5 nerve sheath tumour surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Posterior Cervical Laminoplasty (Bioplate cranial fixation system) and Excision Of C5 nerve sheath tumour surgical procedure.
Spinal nerve sheath tumours (NST), also known as peripheral nerve tumours, are uncommon growths that develop in the covering (sheath) of nerves within the spinal canal or along peripheral nerves branching from the spine. These tumours can occur in different parts of the body but are particularly relevant when they affect the spine.
The two primary types of benign nerve sheath tumours are Schwannomas and neurofibromas. Malignant peripheral nerve sheath tumours are an aggressive and invasive cancer that develop in about 8-13% of patients with NF1. They can also occur sporadically and are associated with a poor prognosis.
Managing spinal nerve sheath tumors often requires a multidisciplinary approach involving neurosurgeons, oncologists, and other specialists to determine the best course of treatment for each individual case. Regular follow-ups are essential to monitor the tumor’s growth and manage any recurrent symptoms.
Indications for surgical treatment should be considered on a case by case basis. There is no good literature on the proportion of cases that require surgical treatment. However, in all cases the option of surgery should be considered and normally surveillance imaging is required if conservative management is pursued.
Apart from malignant transformation the indications for surgical treatment are in the main the development of a progressive radiculopathy, spinal cord extension and rapid growth of the tumour.
Nerve sheath tumours in the cervical spine are most often approached from posteriorly as this allows easy visualisation of the critical neural structures and less risk to the vertebral artery.
There are several variations on the posterior approach, including formal laminectomies or laminoplasty, when the bone is replaced. The advantages of laminoplasty are thought to be restoration of spinal stability and lower risk of late progressive kyphosis. This is the approach described here.
There are a variety of laminoplasty implant options available on the market. In this case simple titanium mini plates are used to fashion a laminoplasty.
Bioplate fixation is with self-drilling screws and two hole straight plates, the screws and plates are made from titanium. The screws are available in 1.9mm and 1.5mm lengths.
If there are concerns regarding spinal stability there is also the option to perform a posterior instrumented fusion. This was not deemed necessary in this case.
OrthOracle readers will also find the following associated instructional techniques of interest:
Cervical laminectomy and resection of spinal cord tumour
Cervical Laminoplasty for treatment of Cervical spondylotic myelopathy
Posterior Cervical Decompression and Fusion using DePuy Mountaineer Instrumentation
Cervical spine decompression: Posterior approach (Degenerative cervical myelopathy).
(With thanks to Navin Furtado FRCS whose case is demonstrated)
Author: Mark Nowell FRCS
Institution: Southmead Hospital, Bristol, UK.